

Anatomy
Cranial Nerve Lesions
Oculomotor (CN III) palsy with sparing of the pupillary reflex is most likely caused by which of the following:
Answer:
Compressive causes of CN III palsy cause early pupillary dilatation because the parasympathetic fibres run peripherally in the nerve and are easily compressed. In diabetes mellitus the lesions are ischaemic rather than compressive and therefore typically affect the central fibres resulting in pupillary sparing.Cranial Nerve III: Oculomotor Nerve
Anatomy / Cranial Nerve Lesions / Head and Neck / Orbit and Eye
Last Updated: 11th April 2019
The oculomotor nerve (CN III) is responsible for movements of the eyeball and eyelid.
| Cranial Nerve | Oculomotor Nerve (CN III) |
|---|---|
| Key anatomy | Arises from midbrain, passes through lateral aspect of cavernous sinus, exits skull through superior orbital fissure |
| Function | Motor: innervates four extraocular muscles (inferior oblique, superior, inferior and medial rectus muscles), levator palpebrae superioris muscle (elevation of upper eyelid), sphincter pupillae muscle (pupillary constriction), ciliary muscle (accommodation), efferent pathway of pupillary light reflex |
| Assessment | Eye movements, accommodation, pupillary light reflex |
| Clinical effects of injury | Depressed and abducted (down and out) eye, diplopia, ptosis, fixed and dilated pupil with loss of accommodation and abnormal pupillary light reflex |
| Causes of injury | Tumours, aneurysms (posterior communicating), subdural or epidural haematoma, diabetes mellitus |
Function
The oculomotor nerve is a motor nerve innervating all of the extraocular muscles responsible for eyeball movements (except for the superior oblique and lateral rectus muscles) and the levator palpebrae superioris muscle responsible for elevation of the upper eyelid. It also provides the parasympathetic supply to the sphincter pupillae (pupillary constriction) and ciliary muscle (accommodation).
Anatomical Course
The oculomotor nerve arises from the anterior aspect of the midbrain and then passes forwards between the posterior cerebral and superior cerebellar arteries, very close to the posterior communicating artery. It pierces the dura near the edge of the tentorium cerebelli, and passes through the lateral part of the cavernous sinus (together with CN IV and VI nerves and the ophthalmic division of CN V) to enter the orbit through the superior orbital fissure.
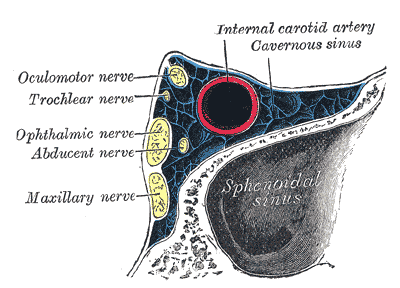
Oblique Section through the Right Cavernous Sinus. (Image by Henry Vandyke Carter [Public domain], via Wikimedia Commons)
At this point it divides into a superior branch innervating the superior rectus and levator palpebrae superioris muscles and an inferior branch innervating the inferior rectus, medial rectus and inferior oblique muscles and supplying parasympathetic innervation to the sphincter pupillae and ciliary muscles. The parasympathetic fibres pass on the periphery of the oculomotor nerve.
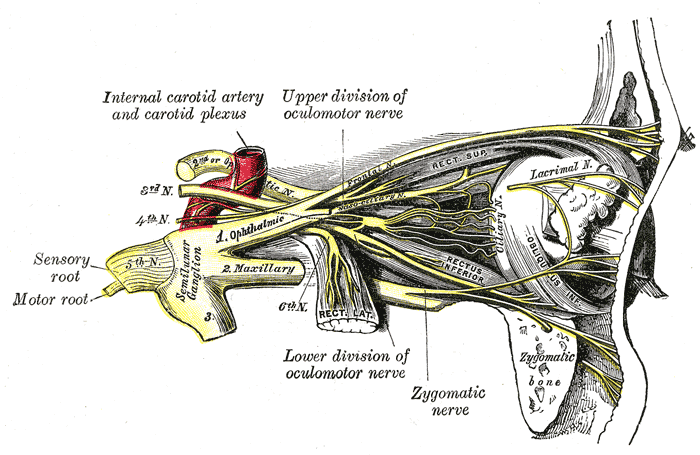
Oculomotor Nerve. (Image by Henry Vandyke Carter [Public domain], via Wikimedia Commons)
Assessment
The oculomotor nerve should be assessed by testing:
- Ocular movements (which also tests the trochlear nerve (CN IV) and the abducens nerve (CN VI))
- Pupillary accommodation
- Pupillary light reflex (which also tests the afferent optic nerve (CN II)).
Likely Causes of Disease or Injury
Causes of CN III palsy:
- Compressive aetiology
- Tumours (commonly by compression against the fixed edge of the tentorium as the medial part of the temporal lobe herniates down)
- Aneurysms (carotid or posterior communicating artery)
- Subdural or epidural haematoma
- Trauma
- Cavernous sinus disease
- Ischaemic aetiology
- Diabetes mellitus
- Hypertension
Compressive causes of CN III palsy cause early pupillary dilatation because the parasympathetic fibres run peripherally in the nerve and are easily compressed. In diabetes mellitus the lesions are ischaemic rather than compressive and therefore typically affect the central fibres resulting in pupillary sparing.
Common Clinical Effects
CN III palsy results in:
- A depressed and abducted eye (down and out pupil) due to unopposed action of the lateral rectus and superior oblique muscles
- Diplopia on looking up and in
- Ptosis
- Fixed pupillary dilatation
- Loss of accommodation (cycloplegia)
- Abnormal pupillary light reflex
- Ipsilateral direct reflex lost
- Contralateral consensual reflex intact
- Contralateral direct reflex intact
- Ipsilateral consensual reflex lost
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |