

Anatomy
Cranial Nerve Lesions
You are teaching a group of medical students about cranial nerve examination. A colleague asks a patient with interesting clinical signs if he would mind being examined. The image below shows the patient after he has been asked to protrude his tongue. Which of the following cranial nerves has been affected:

(Image by Mukherjee SK, Gowshami CB, Salam A, Kuddus R, Farazi MA, Baksh J [CC BY 2.0 (https://creativecommons.org/licenses/by/2.0)], via Wikimedia Commons)
Answer:
In CN XII palsy there is hemiparalysis of the tongue associated with muscle wasting and fasciculations. The tongue deviates towards the weak side upon protrusion due to the unopposed action of the opposite genioglossus.Cranial Nerve XII: Hypoglossal Nerve
Anatomy / Cranial Nerve Lesions / Head and Neck / Mouth and Hard Palate
Last Updated: 11th April 2019
The hypoglossal nerve (CN XII) is a purely motor nerve which innervates muscles of the tongue.
Table: Overview of the Hypoglossal Nerve
| Cranial Nerve | Hypoglossal Nerve (CN XII) |
|---|---|
| Key anatomy | Arises from medulla, exits skull through hypoglossal canal |
| Function | Motor: all intrinsic and extrinsic muscles of tongue (except for palatoglossus) |
| Assessment | Power and symmetry of tongue, tongue protrusion to look for deviation |
| Clinical effects of injury | Hemiparalysis of tongue with wasting and fasciculations, tongue deviation towards weak side |
| Causes of injury | Penetrating trauma, tumours, meningitis, extension of middle ear infection |
Anatomical Course
The hypoglossal nerve arises from the medulla and passes laterally across the posterior cranial fossa within the subarachnoid space before emerging from the cranial cavity via the hypoglossal canal. It then passes inferiorly to the angle of the mandible and moves in an anterior direction to enter the tongue.
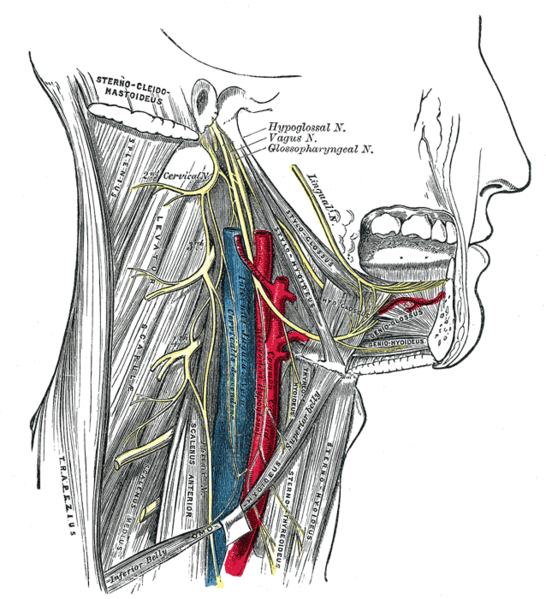
Hypoglossal Nerve. (Image by Henry Vandyke Carter [Public domain], via Wikimedia Commons)
Function
It innervates the hyoglossus, the genioglossus, the styloglossus and all of the intrinsic muscles of the tongue (i.e. all the muscles of the tongue except for the extrinsic palatoglossus muscle innervated by the vagus nerve).
Assessment
The hypoglossal nerve is assessed by:
- Inspecting the tongue for any wasting or fasciculation
- Asking the patient to protrude their tongue to look for deviation
- Testing power of the tongue by asking the patient to push their tongue against their cheek
Likely Causes of Disease or Injury
Isolated hypoglossal nerve injury is relatively uncommon. Possible causes include penetrating traumatic injuries, tumours (e.g. metastases, neurofibroma, cerebellopontine angle lesions), meningitis and infection from the middle ear spreading into the posterior fossa.
Common Clinical Effects
In CN XII palsy there is hemiparalysis of the tongue associated with muscle wasting and fasciculations. The tongue deviates towards the weak side upon protrusion due to the unopposed action of the opposite genioglossus.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |