

Anatomy
Cranial Nerve Lesions
Regarding the accessory nerve, which of the following statements is INCORRECT:
Answer:
Accessory nerve palsy results in inability to shrug the shoulders and to rotate the head to look at the opposite side to the lesion.Cranial Nerve XI: Spinal Accessory Nerve
Anatomy / Cranial Nerve Lesions / Head and Neck / Neck
Last Updated: 11th April 2019
The spinal accessory nerve (CN XI) is primarily a motor nerve innervating the sternocleidomastoid and the trapezius muscles which mediate head and shoulder movement.
Table: Overview of the Spinal Accessory Nerve
| Cranial Nerve | Spinal Accessory Nerve (CN XI) |
|---|---|
| Key anatomy | Originates from cervical segments C1 – C5/C6, enters cranial cavity through foramen magnum, travels through posterior cranial fossa and exits skull through jugular foramen |
| Function | Motor: sternocleidomastoid, trapezius |
| Assessment | Test head rotation and shoulder shrug against resistance |
| Clinical effects of injury | Inability to shrug ipsilateral shoulder, shoulder droop, inability to rotate head towards opposite side to the lesion |
| Causes of injury | Metastatic lymphadenopathy in neck, neck dissection surgery, internal jugular vein cannulation, blunt or penetrating neck trauma |
Anatomical Course
It is a unique cranial nerve because its roots actually arise from motor neurons in the upper five segments of the cervical spinal cord. The fibres leave the lateral surface of the spinal cord, joining together as they ascend, and enter the cranial cavity through the foramen magnum forming the accessory nerve. The accessory nerve then continues through the posterior cranial fossa and exits the skull through the jugular foramen before descending in the neck along the internal carotid artery to innervate the muscles.
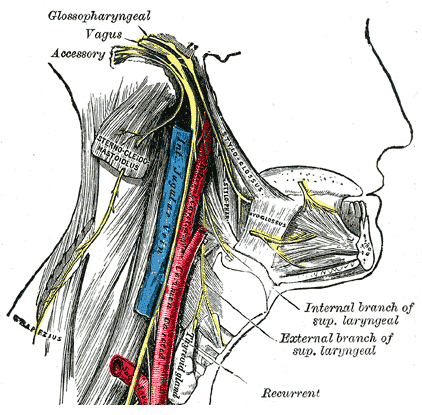
Spinal Accessory Nerve. (Image by Henry Vandyke Carter [Public domain], via Wikimedia Commons)
A few rootlets arising from the medulla just inferior to the fibres that arise to form the vagus nerve, may be referred to as the 'cranial' roots of the accessory nerve. Leaving the medulla these fibres course with the 'spinal' roots of the accessory nerve into the jugular foramen, at which point these cranial roots join the vagus nerve. They are distributed to the pharyngeal musculature innervated by the vagus nerve and are therefore usually described as being part of the vagus nerve.
Assessment
The spinal accessory nerve is assessed by:
- Testing the sternocleidomastoid by asking the patient to turn their head to each side against resistance
- Testing the trapezius by asking the patient to shrug their shoulders against resistance
Likely Causes of Disease or Injury
Damage can occur due to:
- Metastatic disease in the neck with lymph node involvement
- Neck dissection surgery
- Cannulation of the internal jugular vein
- Blunt or penetrating neck trauma
Common Clinical Effects
Clinical features of CN XI palsy include muscle wasting and paralysis of the sternocleidomastoid and trapezius muscles resulting in the inability to rotate the head to the side opposite the lesion and to shrug the ipsilateral shoulder (resulting in shoulder droop) respectively.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |