

Anatomy
This was previously featured in an exam
Abdomen
A 35 year old male is brought to ED with a knife wound. Imaging shows damage to the superior mesenteric artery. Which of the following structures would most likely be affected by this injury:
Answer:
The superior mesenteric artery supplies the midgut structures including the caecum, appendix, ascending colon and proximal two-thirds of the transverse colon. The descending colon and sigmoid colon are supplied by the inferior mesenteric artery.Large Intestine: Colon
Anatomy / Abdomen / Gastrointestinal Tract
Last Updated: 4th August 2022
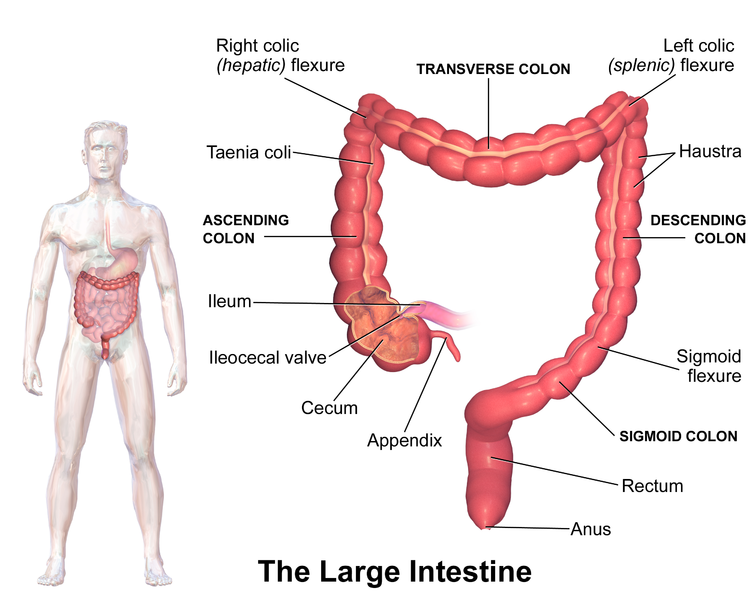
Large Intestine. (Image by Blausen.com staff. “Blausen gallery 2014”. Wikiversity Journal of Medicine. DOI:10.15347/wjm/2014.010. ISSN 20018762. (Own work) [CC BY 3.0 , via Wikimedia Commons)
Anatomical Position
The colon continues from the caecum in the right groin as the ascending colon, which passes upwards through the right flank and into the right hypochondrium.
Just below the right lobe of the liver, it bends to the left forming the right colic flexure (hepatic flexure), and crosses the abdomen as the transverse colon to the left hypochondrium. The transverse colon is related superiorly to the liver, gallbladder, greater curvature of the stomach and the lateral end of the spleen.
At this point, just below the spleen, it bends downwards forming the left colic flexure (splenic flexure) and continues as the descending colon through the left flank and into the left groin. The splenic flexure is higher and more posterior than the hepatic flexure, and is attached to the diaphragm by the phrenicocolic ligament.
The colon enters the upper part of the pelvis as the sigmoid colon, which begins above the pelvic inlet and extends to the level of vertebra S3 where it is continuous with the rectum. This S-shaped structure is quite mobile except at its proximal and distal end which are attached to the descending colon and rectum respectively. Between these points, it is suspended by the sigmoid mesocolon.
The ascending and descending segments are retroperitoneal and the transverse and sigmoid segments are intraperitoneal.

Surface Markings of the Large Intestine. (Image by Henry Vandyke Carter [Public domain], via Wikimedia Commons)
Relations
Table: Anatomical Relations of the Colon
| Colon | Anterior Relations | Posterior Relations |
|---|---|---|
| Ascending colon | Small intestine, greater omentum, anterior abdominal wall | Iliacus and quadratus lumborum, right kidney |
| Transverse colon | Liver, gallbladder, stomach, greater omentum, anterior abdominal wall | Second part of duodenum, head of pancreas, upper end of mesentery, duodenojejunal flexure, coils of jejunum and ileum |
| Descending colon | Small intestine, greater omentum, anterior abdominal wall | Iliacus and quadratus lumborum, left kidney |
| Sigmoid colon | Bladder, uterus and upper vagina | Rectum, sacrum, ileum |
Blood supply
The arterial supply to the colon is derived from the superior mesenteric artery (caecum, appendix, ascending colon, hepatic flexure, proximal two-thirds of transverse colon) and the inferior mesenteric artery (distal one-thirds of transverse colon, splenic flexure, descending colon, sigmoid colon).
As the terminal vessels of the superior mesenteric and inferior mesenteric artery approach the colon they split into many colic branches which anastomose with each other. These anastomoses form a continuous arterial channel which extends the length of the colon, the marginal artery.
At the junctional area of the supply of the superior and inferior mesenteric arteries, the anastomosis may not be sufficient, thus the splenic flexure is most susceptible to ischaemia.
Innervation
The visceral pain sensation from the ascending and transverse colon travels through the lesser splanchnic nerve to the T10 - T11 spinal cord segments hence pain is referred to the umbilical and hypogastric regions.
Pain from the descending and sigmoid colon is carried in the lumbar splanchnic nerves to the L1 and L2 spinal cord segments hence pain is referred to the inguinal region and thigh.
Report A Problem
Is there something wrong with this question? Let us know and we’ll fix it as soon as possible.
Loading Form...
- Biochemistry
- Blood Gases
- Haematology
| Biochemistry | Normal Value |
|---|---|
| Sodium | 135 – 145 mmol/l |
| Potassium | 3.0 – 4.5 mmol/l |
| Urea | 2.5 – 7.5 mmol/l |
| Glucose | 3.5 – 5.0 mmol/l |
| Creatinine | 35 – 135 μmol/l |
| Alanine Aminotransferase (ALT) | 5 – 35 U/l |
| Gamma-glutamyl Transferase (GGT) | < 65 U/l |
| Alkaline Phosphatase (ALP) | 30 – 135 U/l |
| Aspartate Aminotransferase (AST) | < 40 U/l |
| Total Protein | 60 – 80 g/l |
| Albumin | 35 – 50 g/l |
| Globulin | 2.4 – 3.5 g/dl |
| Amylase | < 70 U/l |
| Total Bilirubin | 3 – 17 μmol/l |
| Calcium | 2.1 – 2.5 mmol/l |
| Chloride | 95 – 105 mmol/l |
| Phosphate | 0.8 – 1.4 mmol/l |
| Haematology | Normal Value |
|---|---|
| Haemoglobin | 11.5 – 16.6 g/dl |
| White Blood Cells | 4.0 – 11.0 x 109/l |
| Platelets | 150 – 450 x 109/l |
| MCV | 80 – 96 fl |
| MCHC | 32 – 36 g/dl |
| Neutrophils | 2.0 – 7.5 x 109/l |
| Lymphocytes | 1.5 – 4.0 x 109/l |
| Monocytes | 0.3 – 1.0 x 109/l |
| Eosinophils | 0.1 – 0.5 x 109/l |
| Basophils | < 0.2 x 109/l |
| Reticulocytes | < 2% |
| Haematocrit | 0.35 – 0.49 |
| Red Cell Distribution Width | 11 – 15% |
| Blood Gases | Normal Value |
|---|---|
| pH | 7.35 – 7.45 |
| pO2 | 11 – 14 kPa |
| pCO2 | 4.5 – 6.0 kPa |
| Base Excess | -2 – +2 mmol/l |
| Bicarbonate | 24 – 30 mmol/l |
| Lactate | < 2 mmol/l |