
Revision Resources
May FOAMed
Missed Testicular Torsion
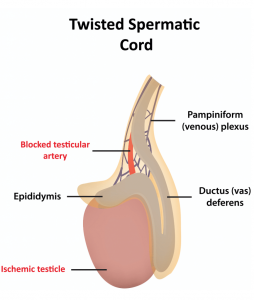
An adult male patient presents to a free-standing ED with RLQ abdominal and flank pain (He claims that he told the triage nurse that he also had inner thigh and groin pain, but there is no record of that). The ED physician evaluates him using an “Abdominal Pain” template that includes testicular torsion as a potential cause. He does not check the box labeled “Male Genital Exam,” and torsion appears not to have been considered. The patient is discharged with a non-specific diagnosis but returns the next day unimproved. He asks to see the same physician from the day before, who meets him in the waiting room before he can check in. The doctor allegedly “rushes him out,” telling him to go to [a nearby teaching] Hospital because “there is nothing more to do.” There his torsed testicle is removed. The patient files a lawsuit against the ED physician claiming he was treated with “willful and wanton negligence.”
Alcoholic Ketoacidosis

Take Home Points
- Alcoholic Ketoacidosis (AKA) can present with significant acidemia (pH < 7.00). Despite the significant acidemia, patients with AKA can remain alert and lucid despite their severe metabolic derangement.
- Relying on urine ketones for diagnosis can be misleading, as acetoacetate is the primary ketone detected in the urine but not the most common ketone generated in AKA. Given the redox ratio in patients with severe ethanol use disorder, urine ketones may be low or negative, as beta-hydroxybutyrate is the predominant ketone body.
- Treatment consists of thiamine, dextrose, and volume repletion.
- Remember to evaluate for concurrent medical illness: gastritis, pancreatitis, pyelonephritis, pneumonia, sepsis.
Acute Hyperthermia

Often when we see elevated temperatures in the emergency department, our first instinct is to search for an infectious source. However, when body temperatures start exceeding 40.5 degrees, infection is a less likely etiology and there are a plethora of conditions that need to be considered.
Polyarteritis Nodosa
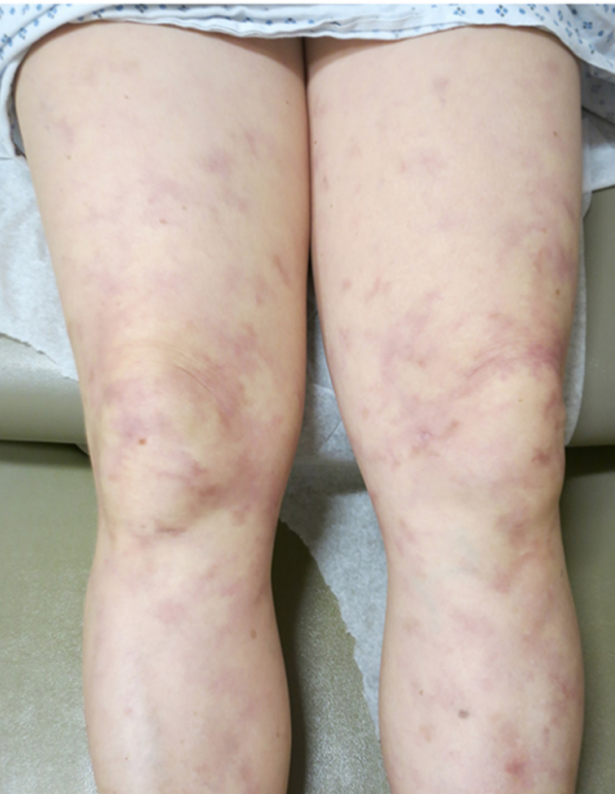
A 59-year-old male presents to the ED with abdominal pain, hematuria, and rectal bleeding for the 5 days. His symptoms have been associated with unintentional weight loss, intermittent fevers, skin rash, and fatigue over the past 3 months. He has a past history of hepatitis B, hypertension, diabetes, and hyperlipidemia. Vital signs include blood pressure 162/103 mm Hg (last measured 118/82 5 months ago, per records), HR 101, RR 18, SpO2 98% on room air. Exam is notable for generalized abdominal tenderness, guaiac positive stool, and generalized purpuric rash over bilateral lower extremities. Labs demonstrate Cr 2.9 (baseline 1.1) and elevated ESR and CRP.
What is the most likely diagnosis, and what are the next steps in management?