
Revision Resources
February FOAMed
Infectious Diarrhoea

Diarrhea is no joking matter (although it can be the butt of many jokes – see what I did there?). It causes a large burden to patients (ex, dehydration), care providers, and the healthcare system. Fortunately, more often than not, it is a self-limited process that requires focusing on maintaining hydration status. There are occasions, however, that may spur one on toward considering antibiotic administration for that “infectious diarrhea.” Recently, the Infectious Disease Society of America (IDSA) published guidelines related specifically to this. So, let’s take a brief moment to review their recommendations on management of Infectious Diarrhea.
The Recurrent Shoulder Dislocation

A 17 year-old football player with prior shoulder dislocation presents to the emergency department reporting shoulder pain after fall. You obtain shoulder x-rays and see the following injury.
What is your diagnosis? Are there any associated lesions you could expect to find? What is your emergency department management?
HIV/AIDS + Fever
A 41-year-old male with history of HIV and poor compliance with medical therapy presents with cough and progressive shortness of breath over several weeks. He noted fever the last several days. His vital signs include HR 114, RR 23, BP 100/56, T 38.1 C, and saturation 88% on room air. He appears toxic.
Stable Angina
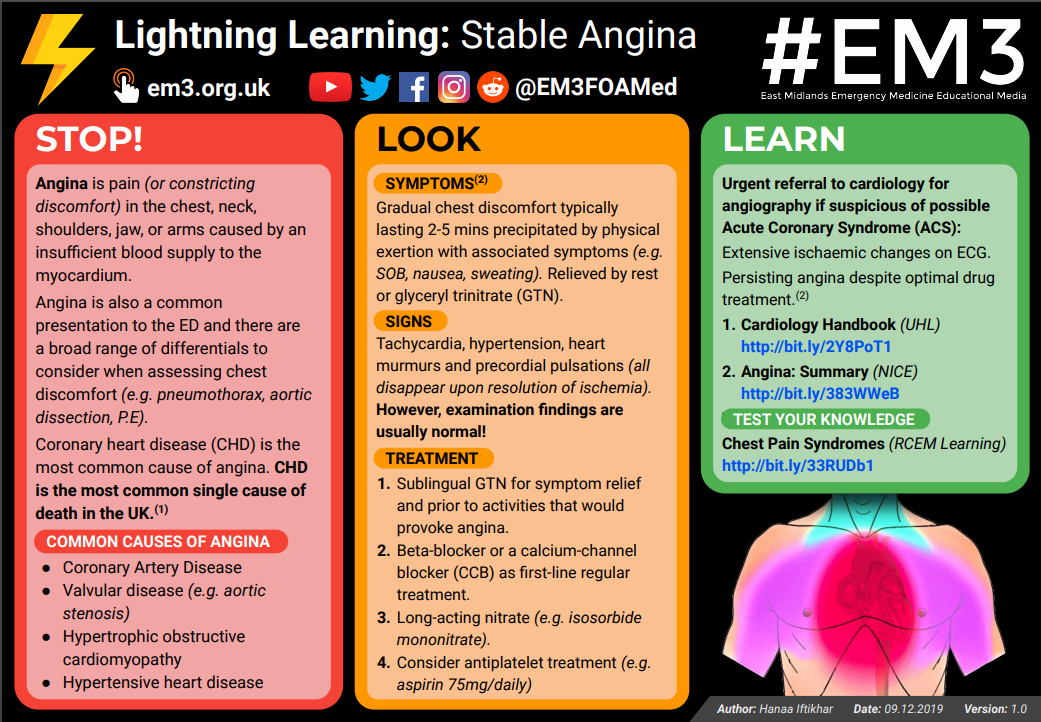
Angina is pain (or constricting discomfort) in the chest, neck, shoulders, jaw, or arms caused by an insufficient blood supply to the myocardium.
Angina is also a common presentation to the ED and there are a broad range of differentials to consider when assessing chest discomfort (e.g. pneumothorax, aortic dissection, P.E).
The latest on Myocardial Infarction

This presentation will give you an update of the current chest pain protocols; including risk scores (HEART, TIMI, EDACS) with / without high sensitive troponin. But also on the newer pathways with rule out of acute coronary syndrome with a high sensitive troponin below the limit of detection or two troponins with a delta.
How do we use these chest pain protocols in tomorrow’s clinical practice? How do you choose a protocol that fits in your institution? Which chest pain patient can we discharge safely from the emergency department and for whom should we organize outpatient follow up? And how do you share your decision with the patient in front of you?