
Revision Resources
August FOAMed
GRACE Guidelines: Approach to Recurrent Low-Risk Chest Pain
In the United States, a patient with chest pain presents to the emergency department (ED) every 5 seconds. By the time you finish reading this post, 60 patients will have sought treatment for chest pain. In 2017, chest pain was the second most common chief complaint in US EDs totaling more than 6.5 million visits, or approximately 2.5x the population of Chicago. There have been dramatic advances in the management of ACS and low-risk chest pain. Prior to the days of observation units, I recall admitting high-risk patients with chest pain to a telemetry floor. However, admissions have changed to observation stays, 6-hour 𝚫 troponins changed to 2-hour 𝚫 troponins, conventional troponins changed to high sensitivity troponins, and much more. Remarkably, up to 40% of patients with chest pain will return to the ED with similar concerns within one year. Yet, there is sparse evidence to address the subset of low-risk patients with recurrent chest pain.
Differential Diagnosis of Ear Pain
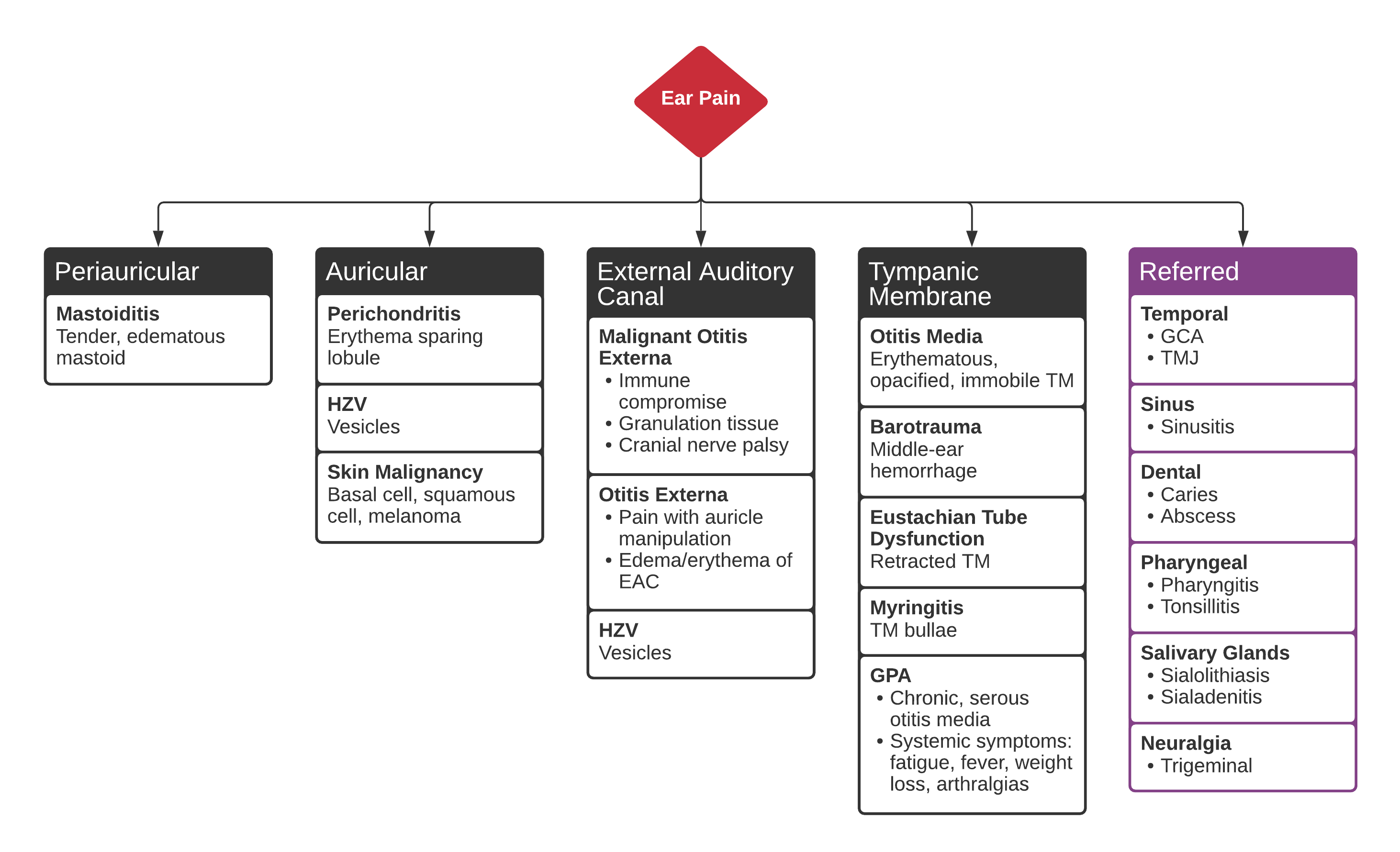
A 48 year-old female with a history of hypertension, diabetes, and hyperlipidemia presents with ear pain and discharge. She notes an associated headache and fevers. Examination demonstrates external auditory canal edema with granulation tissue along the floor. No cranial nerve abnormalities identified.
Heat-Related Illness & First Principles

Heat-related illness is a very common form of environmental injury. Like many insults, it may be modelled by ‘diathesis-stress.’ In other words, heat-related illness materializes at the cross-roads of inherent patient characteristics [e.g., age, co-morbidities, genotype, that is, one’s diathesis] and external stress [e.g., ambient temperature, humidity, exertion]. Thus, those with multiple, chronic co-morbidities, the elderly and children may be more susceptible because they are less able to dissipate heat and maintain oral hydration.
Proctitis
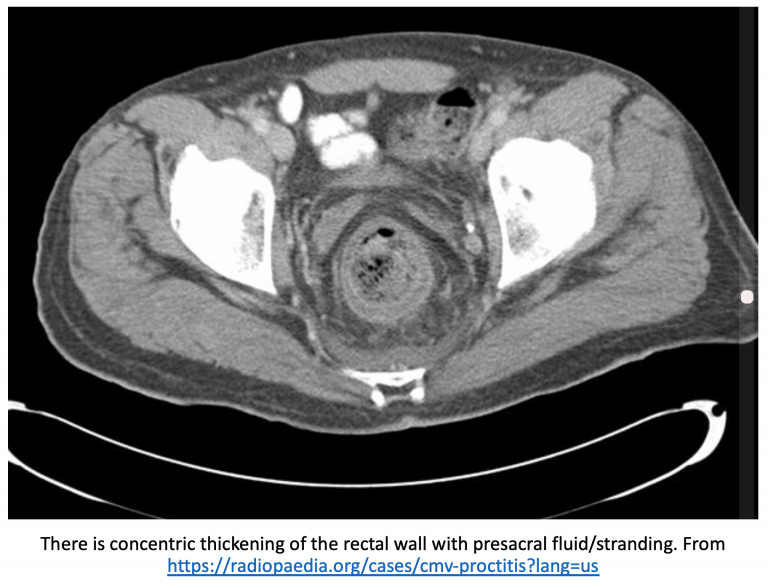
A 42-year-old male undergoing recent radiation therapy for colorectal cancer presents with pelvic and anal pain and pain with defecation. He experiences extreme pain prior to and during defecation. He has had mucous and blood in his stool. He denies a history of hemorrhoids.
Pertinent physical examination findings include tachycardia, temperature 101.2 F, and lower abdominal pain to palpation. Rectal exam reveals no fissures or hemorrhoids, but digital exam reveals tenderness.
What’s the next step in your evaluation and treatment?
Hand Infections in the Emergency Department
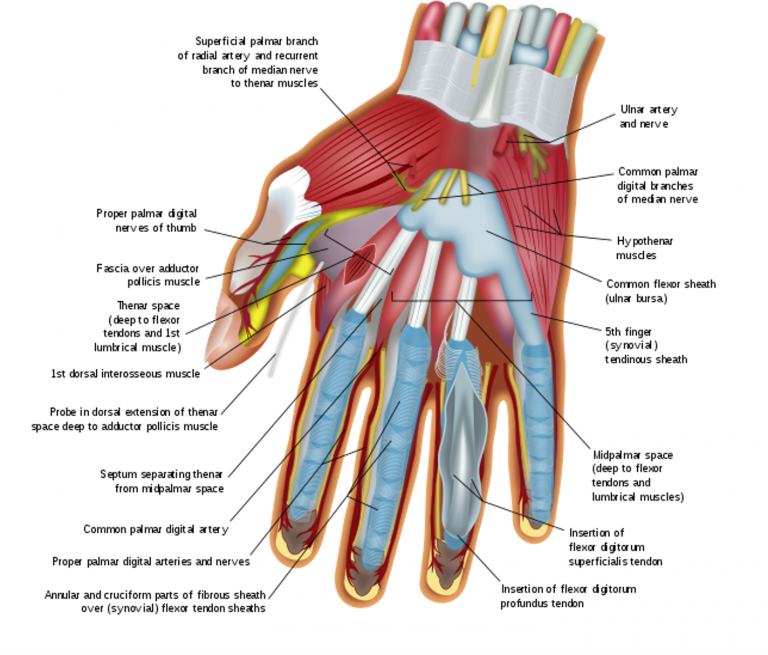
A 23-year-old female with type-2 diabetes presents with a “swollen index finger.” Her cat bit her finger 4 days ago; since then, her finger has become progressively more swollen, red, and painful. The patient developed a subjective fever this morning, and her pain has become excruciating, which is why she came to the Emergency Department (ED).
The patient’s heart rate is 110, her temperature is 101.1F, and the remainder of her vital signs are normal. The patient is diaphoretic and in moderate distress due to pain. Her right index finger is diffusely swollen, with a small puncture wound on the fingertip. The patient is holding the finger in a slightly flexed position, because even minimal extension causes excruciating pain. The entire finger is tender, most prominently on the ventral aspect. The remainder of her exam is normal.